Anatomical Variant of Profunda Femoris Artery : Preliminary report of Femoral CTA study
Suwanbundit A, Sriwilas P, Klaklangchon A. Anatomical variant of profunda remoris artery : preliminary report of femoral CTA study. J Interventional radiology Technicians and Nurses, 2011; 5 (1) : 60-67.
ABSTRACT
Purpose: To determine the varients of profunda femoris artery [PFA] in origin, size and distance to origin by femoral artery CTA imaging.
Materials and Method: Retrospectively review of 117 patients with femoral artery CTA, sites of origins were identified, diameter and distance of PFA.
Results: 234 femoral CTA. Shown 35.9% of PFA were originated from posterior site of Femoral artery, the second were originated from lateral site 33.33% then posterolateral origin was 27.78%. Most of MCFA (62.88%) and LCFA (67.09%) were originated from PFA. The diameter of PFA in Thais were 5.29 mm. and 5.49 mm. , mode of diameter of PFA was 5.1-6.0 mm [38.03%]. The Distance of PFA from the mid point of inguinal ligament to the origin of PFA was 34.29 mm. in the left PFA and 36.29 mm. in the right PFA.
Conclusion: Variant of PFA in which the origin of PFA is posterior side of the femoral artery differed from Boonkham (1987) who studied in Thais cadavers. However most of PFA vessel was originated in lateral side of femoral artery in female both side and male left side.
Introduction
Type of anatomical variation in the origin of profunda femoris artery [PFA] is concern during puncture by seldinger method for cathererization in interventional procedure. Many minor and major complication is reported such as [3][7][9] arterial dissection, hematoma, arterio-thrombosis and pseudoaneurysm due to double side puncture technique or the tip of introducer invade the origin of PFA. Never report is described in the imaging and any suggestion in the performance. However the vascular disease in this location is rare [3][5][6][9] which only case reported.
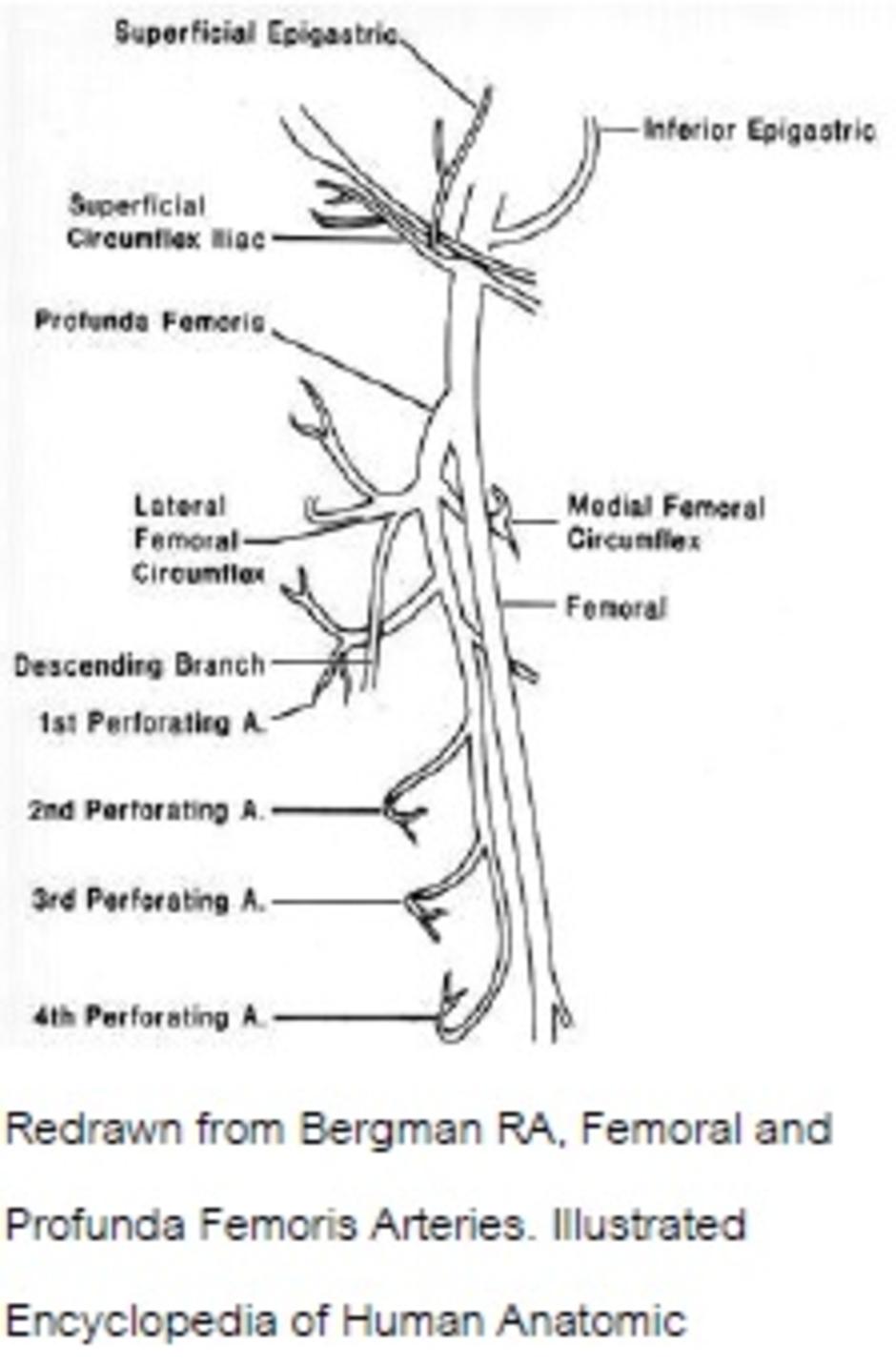
PFA had 4 type were described as type A: PFA arise from posterior side, type B: PFA arise from posterolateral side, type C: PFA arise from lateral side and type D: PFA arise from medial side, many PFA in cadavers is reported as [1][2][8][11]. Pioneer repost in PFA in Thai established type B however the lastest report shown type A [1][12] instead however the report determined by high resolution
The purpose of our study was to determine sites of origins, diameter and distance of PFA
Method
We retrospective reviewed 117 patients (234 side of) femoral artery CTA at Siriraj Hospital, Bangkok, Thailand. Institutional ethical review board approval was accepted our study.

Procedure
Femoral artery CTA were done by CT 64 slices [LightSpeed,GE Medical] with iodinated contrast medium administration for 100 ml. of 370 mgI concentration by automatic injection at 4ml/sec, 300 PSI and serial scan with smart-prep technique. 1.25 mm. of slice thickness and interval then postprocessing with Advantage Workstation version 4.2 were set.
Statistical Analysis
We compared origin, size, distance in Femoral Artery CTA measured by 2 observers (interobserver reliability p<.001), mean, percentage and multivariate statistics were performed. Analyses were performed using the SPSS statistical software [Version 15.0, SPSS Inc., Chicago, IL]. A P- value of less than 0.05 was considered significant. The literature review was obtained to compare our outcome to those others. Literature was searched from Pubmed libraries on electronic databases with the terms of ‘profunda femoris artery’, ‘femoral CTA’ combined with ‘cadavers’ in the period from 1987 to 2010. Reviews and case reports were included.
Result
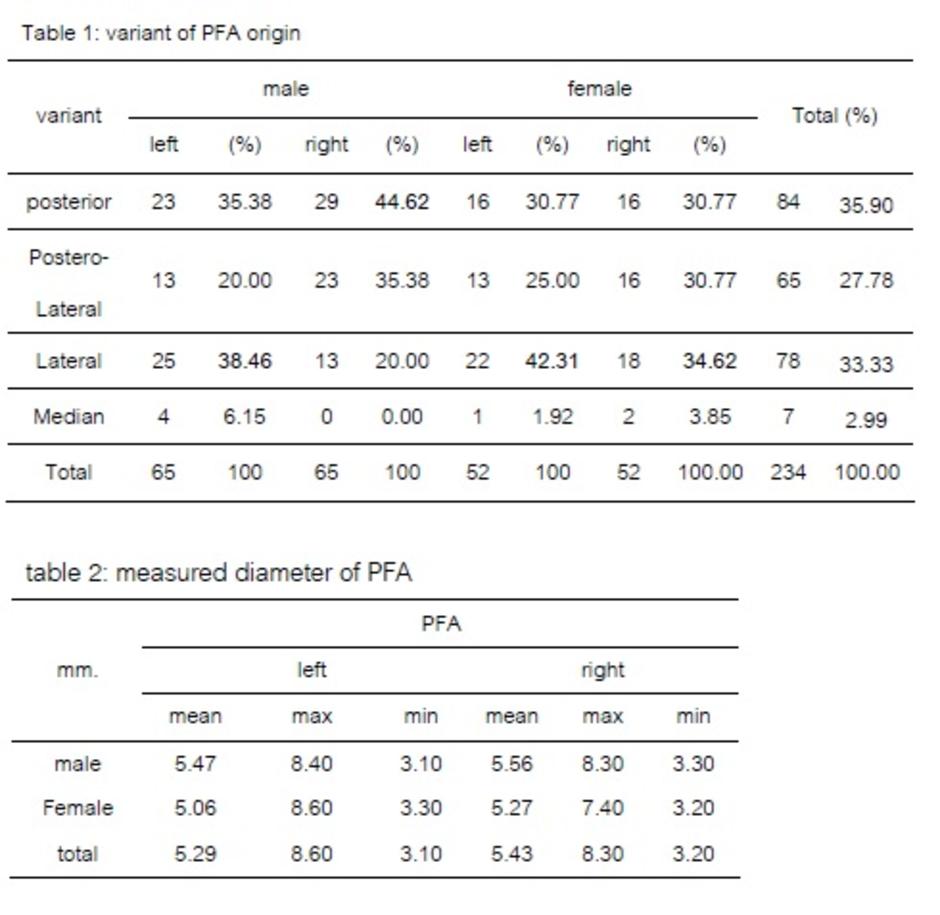
One hundred and seventeen patients [52 females, 65 males, age range from 16-89 years, mean age 62.5 years] with 234 femoral CTA. Of those, 84 of 234 [35.9%] PFA were originated from posterior site of Femoral artery (see table1). The second were originated from lateral site of FA [78/234, 33.33%] while postero-lateral origin was 27.78% [65/234]. Dramatically founded that the origin of PFA was most from lateral side of femoral artery in female both left and right side and male in the left side [42.31%, 34.62%, 38.46%] respectively, whereas the originated from posterior [44.62%] is only greatest numbers of right side of male femoral artery. Only PFA in male which right PFA had statistical significant differences of the origin with left side [p<.011] and with female right PFA [p<.021].
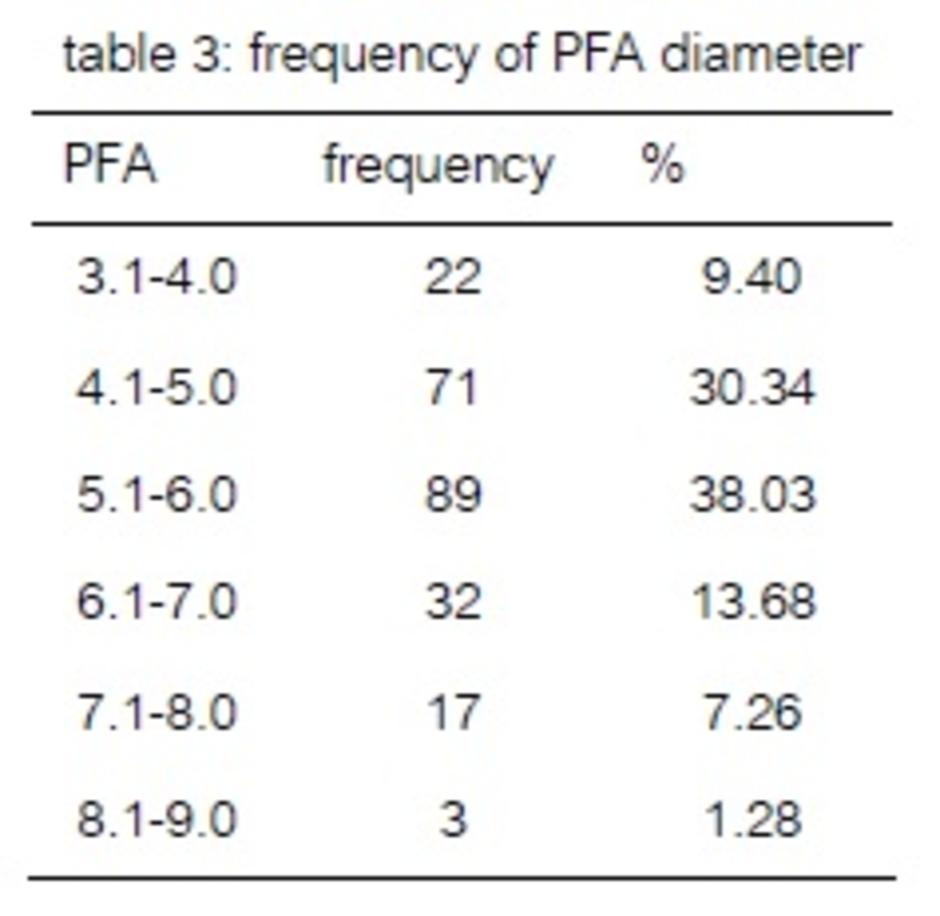
The diameter of PFA in Thais were 5.29 mm. and 5.49 mm. in the left and right PFA respectively (see table4), male had PFA diameter as 5.47mm., 5.56 mm. and female had 5.06 mm., 5.27 mm. side by side accordingly, there was statistical significant differences between sex [male diameter of left PFA was larger than female’s left PFA] at p<.034. Mode of diameter of PFA was 5.1-6.0 mm [38.03%].(see table5).
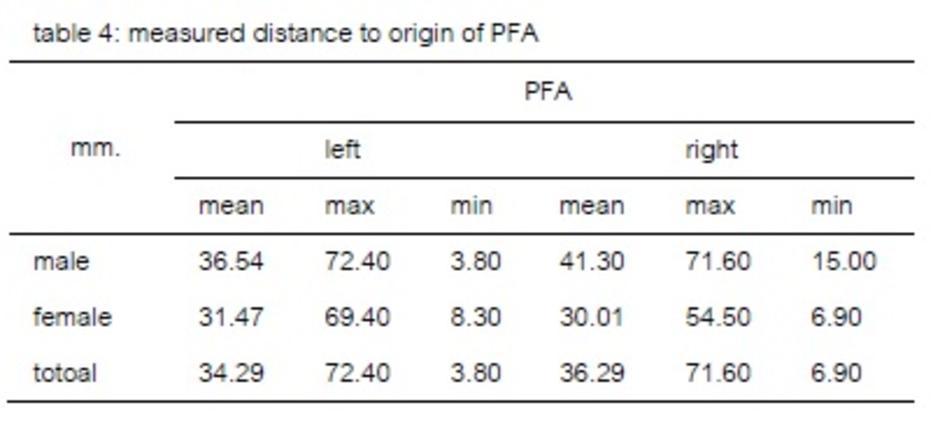
The distance of PFA from the mid point of inguinal ligament to the origin of PFA was (see table6) 34.29 mm. in the left PFA and 36.29 mm. in the right PFA. Male had 36.54mm. and 41.30 mm., female had 31.47 mm.,30.01 mm. side by side. There was statistically significant difference in male right PFA is longer than left, pp<.03 and than right PFA of female at p<.0001
Discussion
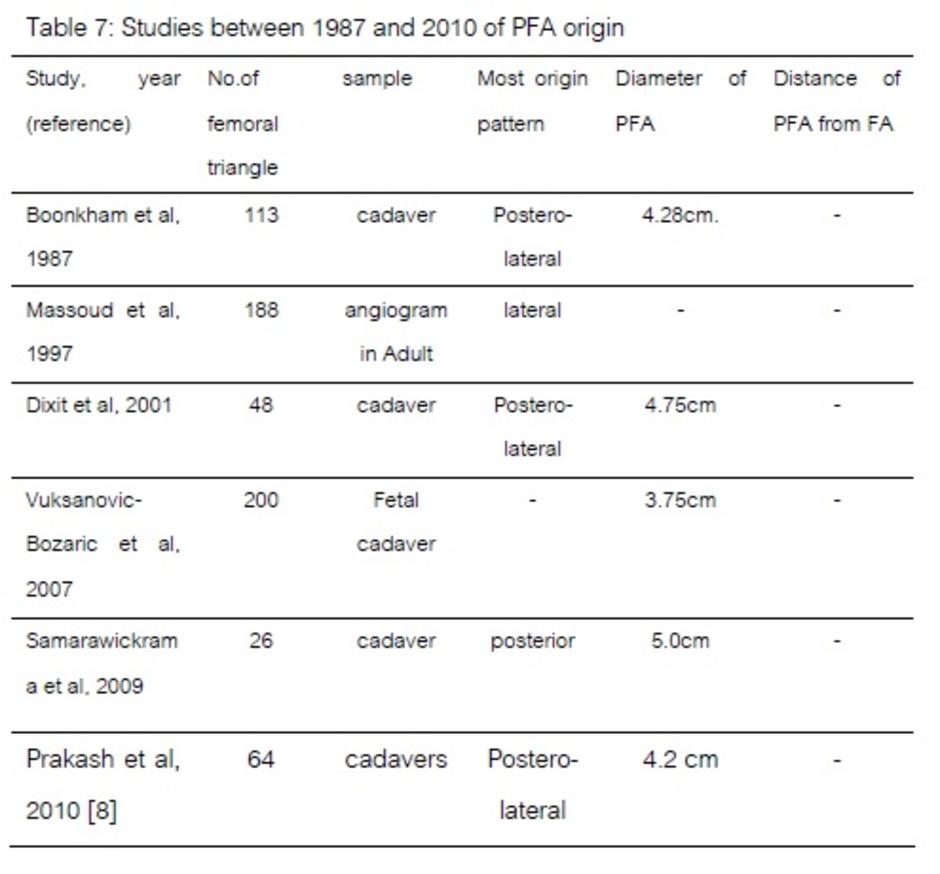
In this study, the CT angiography was provide the quality 3D imaging to study the variant of PFA in which the origin of PFA is posterior side of the femoral artery same as Samarawickrama (2009) but differed from Boonkham (1987) who studied in Thais too. However this research found that most of PFA vessel, determinated by sex and side, was originated in lateral side offemoral artery in female both side and male left side in which the normal puncture site for angiogram is right side ,the interventionist should be concerned about the posterior origin of the right side for the double side puncture technique. However, the distance of PFA from the mid point of inguinal ligament to the origin of right PFA was 36.29 mm. that too short to be the puncture site (2inches below and 2 inches lateral to ligament) but in the introducer insertion sometime can be disturbed this vessel and get complication.
References
- Baptist M. Anatomical variations. Profess med j. 2007; 14(3): 523-7
- Boonkham Y, Plakornkul V. Variational anatomy of the profunda femoral artery in Thais. Siriraj Hosp Gaz. 1987; 39(8): 441-5
- Chitra R. Folia Morphol (Warsz). A rare variational anatomy of the profunda femoris artery. 2008; 67(2): 157-8.
- Chleborad WP, Dawson DL. The profunda femoris artery: variations and clinical applications. Clinical Anatomy. 1990; 3(1): 33-40
- Defraigne JO, Vasquez C, Limet R. Ruptured aneurysm of the profunda femoral artery associated with polyaneurysmal disease. Acta Chir Belg. 1997; 97(2): 93-6.
- Dixit DP, Mehta LA, Kothari ML. Variations in the origin and course of profunda femoris. J Anat Soc India. 2001; 50(1): 6-7
- Dorrucci V, Veraldi GF, Dusi R, Franceschetti ME. [True aneurysm of the profunda femoris artery. Case report and literature review]. Minerva Chir. 1998; 53(10): 847-51.
- Gautier E, Ganz K, Krugel N, Gill T, Ganz R. Anatomy of the medial femoral circumflex artery and its surgical implications. J Bone Joint Surg. 2000; 82(5): 679-83
- Massoud TF, Fletcher EW. Anatomical variants of the profunda femoris artery: and angiographic study. 1997; 19(2): 99-103
- Milotic F, Milotic I, Flis V. Isolated atherosclerotic aneurysm of the profunda femoris artery. Ann Vasc Surg. 2010;24(4): 552.
- Onal B, Kosar S, Gumus T, Ilgit ET, Akpek S. Postcatheterization femoral arteriovenous fistulas: endovascular treatment with stentgrafts. Cardiovasc Intervent Radiol. 2004; 27(5): 453-8.
- Prakash, Kumari J, Kumar Bhardwaj A, Jose BA, Kumar Yadav S, Singh G. Variations in the origins of the profunda femoris, medial and lateral femoral circumflex arteries: a cadaver study in the Indian population. Rom J Morphol Embryol. 2010; 51(1): 167-70.
- Rainio P, Biancari F, Leinonen S, Juvonen T. Aneurysm of the profunda femoris artery manifested as acute groin pain in a child. J Pediatr Surg. 2003; 38(11): 1699-700.
- Samarawickrama MB, Nanayakkara BG, Wimalagunarathna KWR, Nishantha DG, Walawage UB. Branching pattern of the femoral artery at the femoral triangle: a cadaver study. Galle Med J. 2009;14(1): 31-34
- Shakeri A, Tubbs RS, Shoja MM, Ghabili K, Hashemzadeh S, Oakes WJ. Analysis of the profunda femoris artery with superficial femoral artery occlusive disease. Biomed inter.2010; 1: 62-65
- Vuksanovic-Bozaric A, Stefanovic N, Pavlovic S, Duraskovic R, Randelovic J. Analysis of deep femoral artery origin variances on fetal material. Facta Univ. 2007; 14(3): 112-6