เรามา...ช่วยกัน....ดูแลน้อง...ในครรภ์ ...ร่วมกันนะคะ..เธอยิ้มได้...เธอยิ้มออก
SHA คือ..ความสุข...ในการทำงาน ... เราทำงาน .. "ด้วยใจ" ...เราทำงาน.. "ด้วยความสุข" .... สิ่งที่เรามอบให้คนอื่นนั้นก็..คือ ... ความสุข ...ที่พวกเขา/คนไข้...จะได้รับ ... ซึ่งคำตอบและมองได้จาก... "รอยยิ้ม" .... ที่หมอเปิ้นได้รับจาก... "แม่วัยใส" ... เมื่อได้ลงไป ... เยี่ยมบ้านพวกเธอ และ ไปดูแล/พูดคุยกับเธอ...ที่บ้าน (Home Visit & Home Help Care) ... อยู่เสมอๆๆ มาค่ะ .... พวกเธอบอกว่า ... หมอเปิ้น....ได้ช่วย...."บรรเทาความทุกข์".... ของเธอ ... ได้...ช่วยลดแรงปะทะ และ แรงกดดัน....จาก..ครอบครัว... จาก...คนในชุมชน และ จากโรงเรียน .... นะคะ ... คำตอบนี้ ...วัดได้จาก ... "รอยยิ้ม และ น้ำตา" .... ของพวกเธอค่ะ

ออกไป...เยี่ยมบ้าน ... รถเข้าไปไม่ถึงค่ะ..... เราต้องเดินเข้าไป.... เดินไปหา...พวกเธอ...ไปกันนะคะ (ซึ่ง.. "ใจเป็นนาย"... กายเป็นบ่าว นะคะ)


เราเข้าไป...ไปติดตาม..หลายๆเรื่องค่ะ... การเลี้ยงลูกด้วยนมแม่... ติดตามด้านจิตใจและอารมณ์ (Mind & Emotion)
"Innovative depression prevention in Thai adolescent mothers during pregnancy."
Somsri Nawarat
Banlad Hospital
Petchaburi Province, Thailand,






IV. results ==> "Innovative depression
prevention in Thai adolescent mothers during pregnancy"
The research findings are reported as follows. First, this research study suggested the model called “Teen Moms Care Model” which consisted of “1D4S”
(Depression, Somatic and medical support, Social support, Self-esteem and
Stress). Second, the structural equation model of the variables affecting
the depression in pregnant Thai adolescents as per the hypotheses or conceptual
framework of the study corresponded with the empirical data. The researcher
adjusted the model six times. The results of testing statistical data of the
adjusted structural equation model and the standard criteria suggested by Joreskog&
Sorbom
(1996) reported that all of the
statistical data of the model passed the standard criterias: Relative χ2(χ2/ df)= 1.61, Goodness of Fit Index(GFI)= 0.96, Adjusted Goodness of Fit Index(AGFI)= 0.94, Root Mean Squared
Residuals (RMR) = 0.023, Standardized Root
Mean Squared Residual(SRMR)=
0.042,Root Mean Squared Error of Approximation(RMSEA)=
0.038, p-value for test
of close fit= 0.94, Normed
Fit Index (NFI)=0.98, Incremental Fit Index
(IFI)= 0.99, Comparative Fit Index(CFI)=
0.99, Critical N (CN)=295.80.
However, the findings suggested thatLikelihoodRatio
Chi-SquareStatistic(c2)is
still statistically significant because it is sensitive to multivariate
normality. If the sample size is small, the tested statistical data
distribution is always not close to c2standard distribution. In contrast, if the sample size is
too big, the df model is always rejected. Therefore, theLikelihoodRatio Chi-SquareStatistic(c2) remains problematic. The estimation of model in this
research used Relativec2(c2/df)instead.
The findings from the study the direct effect, indirect
effect and total effect of the variables affecting depression in
418 Thai adolescent mothers during pregnancy showed that somatic and medical support had a positive direct effect
and a negative indirect effect towards depression with the coefficient of 0.16
and -0.14 respectively but had no overall effect. Self-esteem had no direct
effect but had an indirect and negative overall effect with the coefficient of
0.31 and -0.47. Social support had no direct effect but had an indirect effect
and negative overall effect with the coefficient of -0.30 and -0.27. Stress had
a positive direct effect and positive overall effect towards depression at the
effected coefficient of 0.84 but had no indirect effect at the statistical
significance of 0.05as per Figure 7 and Table 1.
TABLE 1: THE ANALYSIS OF PARAMETER, DIRECT,
INDIRECT, TOTAL EFFECTED COEFIFICIENTS
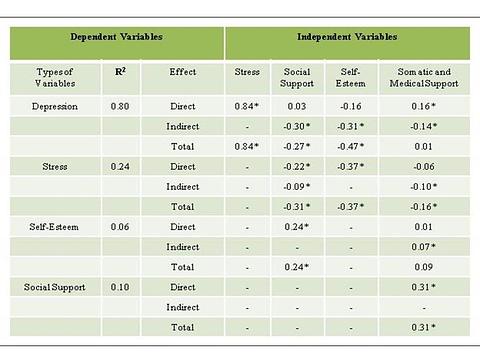
*
means the statistical significance at 0.05

FIGURE 5 THE STRUCTURAL EQUATION MODEL OF THE VARIABLES AFFECTING THE DEPRESSION (ADJUSTED MODEL)
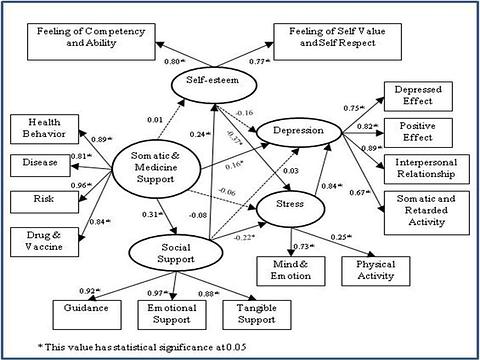
According to Figure 3,the structural equation model of the variables affecting the depression in pregnant Thai adolescents in Phetchaburi province depicts the model called “Teen Moms Care Model” which consists of “1D4S” (Depression, Somatic and Medical Support, Social Support, Self-Esteem and Stress). Meanwhile, the in-depth analysis of qualitative research with the variable of somatic and medical support report that the pregnant adolescents have food consumption misbehavior and malnutrition. They eat what they like, for example, they do not like drinking milk but soft drinks. They prefer pickled fruits and vegetables to the fresh ones. This results in the risk of under-weighted and pallid children. The negligence of taking care of their health and the suggestions of doctors on taking iron and iodine supplements, rejecting food necessary for increasing blood concentration, and rejecting sea food to supplement iodine lead to lacks of iodine and disease protection. Furthermore, the problem of Rh negative blood group also found in 2 subjects while 99% of Thai people have Rh positive, and two adolescent mothers who carried twins must have caesarean section. The heights of 3 adolescent mothers do not reach 150 cm. which represents prematurity. The youngest adolescent mothers found aged only 12 years old. For the self-esteem variable, during the in-depth interview, the researcher found that the pregnant adolescents felt that they were wrong and misbehave because they were pregnant while they were students. More than half of the samples said that they were studying in secondary school and high school. Their self-esteem level was lower because they had to quit school, they felt that they were useless, ashamed to friends, teachers, local people, had negative self-perception, unsatisfied with their pregnancy, made their parents upset, ashamed and lack of social acceptance. They had to change their roles from students to mothers when they did not want to be, and they had negative self-perception. Eight adolescent mothers were not accepted by their husbands. Eleven adolescent mothers did not know before that they became the second or third wives. Some of them took the abortion pills. When they found that they did not have menstruation, they were sure that they were pregnant then they had very high stress. They did not receive good care from their husbands even giving money for taking care of the children, asking them how they had been, or boosting their spirits. Most of them were supported by the society and most of the helps came from their mothers and grandmothers in terms of accommodation, comforting, caring, and taking them to the hospitals for checking as per the doctors’ appointments.
For the stress variable, the findings report that when the adolescents know that they are pregnant, they have very high stress. They cannot sleep well, worried, unhappy, and afraid of misconduct. They are scared to tell anyone and want to die especially when they know that they become the second or third wives. They lack concentration, some of them escaped from their families, schools, and have headaches. Some of them conceal the pregnancy for 5 months and their husbands do not accept the responsibility to become a father of the baby. They feel very unhappy and hide from their parents, schools, friends which lead to depression. When they know that they are pregnant, they do not want to talk to anyone, feel bored, upset, and unhappy, feel lonely, cry every night, cannot sleep well, and have nightmares. They would like to be by themselves, do not want to meet anyone and escape from their families. They are afraid of being gossiped and scared of the delivery process. They want to die and think about committing suicide. The depression caused by accumulated stress cannot be solved, they are unhappy both physically and mentally, they are too ashamed to meet anyone, and they cannot earn their living. Their husbands are also students and they still have to ask their parents for money. Therefore, the pregnant adolescent mothers have many problems on somatic and medical support, self-esteem, and social supportwhich lead to stressand depression.
In general, the finding of the structural equation model of the variables affecting the depression in pregnant Thai adolescents in Phetchaburi province suggested the model called ....“Teen Moms Care Model” which consisted of “1D4S” such as somatic and medical support variable with the factors consisting of health behavior, risk, disease, drug and vaccine.

The findings in this study correspond with those previous studies. In terms of risk, the pregnant adolescents younger than 17 years old have anemia, malnutrition, late and incomplete Ante Natal Care, urinary tract infection, the size of the babies are not appropriate for the pelvic bones, and miscarriages caused by self-abortion (Ukrit Uchupap, 2010; Bunpode Suwannachatand Prapatsorn Ualalitchoowong,2007). The pregnant adolescents aged 13-17 years old face with the height and weight lower than standard, abortion, poor living condition, smoking, drinking alcohol, drug addiction, urinary tract infection, thyrotoxicosis,malnutrition,anemia, twins pregnancy, no Ante Natal Care. Their ages are lower than WHO pregnancy criteria. They never have birth control, so they are unintentionally pregnant and not ready. The adolescent pregnancies are constantly increased and the ages of adolescent mothers are lower and lower compared to the past. The rate of caesarean section increases with the complications. Most of the adolescent mothers are unemployed, have the abortion background, never have marriage ceremony. They are mistreated and are the victims of physical and sexual violence, abusive by their husbands, and they have low income. (White, 2004; Wasan Watewatanachai, 2007; Suradet Boonyawet,Chiraphorn Mongkhonprasoet and Rattana Ngamboonyarak, 2007; Lapvongwatana, 2000)
Regarding self-esteem, the findings of this study correspond with previous studies that the pregnant adolescents never have marriage ceremony and have premature sexual intercourse. The adolescent pregnancy reduces self-esteem of those young mothers and ends their teenage lives. They have to quit school and they are unemployed which lead to drug addiction and low self-esteem (Nirattharadorn, 2005; Srisaeng, 2003; Spears, 2007). The self-esteem is low, lack of self-image and good birth control, poverty, illiteracy, no inspiration/ Besides, they cannot adapt themselves to the new role of a mother. Facing with social problems, bad communication, pregnant adolescents possess low self-esteem (Neamsakul,2008; Byrn, 2011).
In terms of social support, the results this study support those of the previous studies that the adolescent mothers move from their homes, face with negative interaction and sarcastic words from people around them. People often look at them strangely and gossip them. They change their roles from students to mothers. They feel ashamed since they have changed their roles from being daughters to adolescent mothers, from being the girls who work in the factory to unemployed pregnant girls. They face problems of negative attitude towards life style, economy, low social support, lack of helps from husbands and families, abuse, and unemployment. The first-time mothers do not have any knowledge about how to take care of the babies and themselves. They are sexually harassed, abandoned by husbands and their husbands do not accept the responsibility to be a father. Their low social esteem further leads to negative behaviors like drinking alcohols, drug addiction, and attempt to commit suicide. They become homeless, are forced to leave home, quit school, do not have food and money, perform illegal conduct, and commit crime (Kohorn, 2011;Neamsakul, 2008; Ruppel,2001; Rebekah, 2008). The findings also show that the pregnant adolescents have to live with their husbands on their own. They become malnutrition, do not have money and social support, depressed, abused, suffer from sexual harassment, abandoned by their husbands, have negative attitude towards pregnancy, have bad health behavior, low education, and low self-esteem. Peer group has strong influence on pregnancy, poverty, lack of food security, negative events in their lives, physical violence, sexual harassment, earning problem, emotional suffer, low quality of living, and bad attitude towards becoming mothers. They do not get any supports from husbands, families, peer group, lack of medical information and no mental help which affects how to improve the quality of life of the pregnant adolescents. These factors are in correlation with social support of adolescent mothers both during pregnancy and after giving birth. The adolescent mothers do not pay attention to nutrition, consumption, inappropriate eating habit on meals, quality, and quantity of food. They do not get any support of necessary items and facilities. They also have relationship problems with their families. These are important to the practice of taking care of the pregnant adolescent health. (Kimberly, 2009;Vo, 2008;Clutter,2009; Chrzan, 2008; Hagelskamp, 2011).
For the stress variable, this study correspond with the studies of many researchersthat the stress variable of the pregnant adolescents caused by the change of their roles to become mothers but they cannot accept this reality. They are ashamed, have to quit school, receive negative feedback from society, afraid of delivery. The blame from their parents and the pregnancy while they are students result in no money and unemployment, they also feel unhappy and have high stress. They are 15-19 years old girls, they fail to control their emotions and express negative emotions. The blame from their parents results in high stress and bad mental health that leads to depression (Boland-Prom, Kimberly Wynn,2004). In the meantime, the findings also show that adolescent mothers are not doing well with stress, coping with stress, and adapting themselves during pregnancy. Becoming a mother unintentionally causes suffering from pregnancy, blemishes, and failure to adapt. Some of them use negative strategy by escaping from the society, over consuming food, using drugs, smoking, getting low social support, experiencing high level of loneliness, having low economic status in the society, and feeling unhappy. These result in stress of the adolescents throughout pregnancy period (Borcherding, 2005; Golden, 2006;Smith, 2007).
In terms of depression, this study corresponds with the previous studies in that life style factor of the pregnant adolescent is in correlation with depression. They have stress, smoke and drink alcohol, use drugs, conflict with their family members, suffer from bad events in their lives. They also have problems with marital status because they are unintentionally pregnant while they are still young and have low education level, abused by family, face with negative interaction from their partners and family members, negative behavior from society, and change in roles. The findings suggest that family can help pregnant adolescents in 3 aspects: their future, drug problems, and ability to cope with the undesired pregnancy. These result in reduction of depression, stress, risk of committing suicide, economic and social problems, occupation and income of adolescent mothers(Hanson, 2001; Lapvongwatana, 2000; Creelman,2002;Jean,2005;Gosdin, 2010; Gavin,.2004;Meighan, 2006). Moreover, the findings also show that the pregnant adolescents are worried and have emotional instability which are in correlation with socio economic status, physical health, the number of people whom they live with, work, risky behavior, their behavior during pregnancy, alcohol drinking, income, poverty, social status, financial status, GPA, education level, life style, fear of giving birth, blemishes, cigarette smoking, marijuana smoking, malnutrition, unplanned and undesired pregnancy, abortion, negative interactions from their partners and family members, low self-esteem, and attempt to commit suicide. Social and cultural factors are in correlation with the depression in adolescent mothers. (Feltes, 2007;Sountorp.2007;Warren, 2008;Gosdin, 2010; Wanna Kongsuriyanavin, Benjawan KhunrattanaponandKittirat Techatraisak, 2010;Byrn, 2011;Meighan, 2006; Shelton, 2011;Angela, & Ekwonye 2011).
วันนี้ หนูเปิ้น .... นำเสนอแค่นี้ก่อน...นะคะ ... แม่ต้อย คนสวย

เธอ....อายุ 14 ปี เรียนอยู่ ม. 2 และ สามี และ..ครอบครัวของสามี "ไม่ยอมรับเธอและลูก"




สร้างความเข้าใจ + ใสใจ...และตามไป...เยี่ยมที่บ้าน นะคะ

คุยปัญหาต่างๆๆ ...ที่เธออยากเล่า ....เล่า...เพื่อเธอ จะได้ระบายและ...เธอสบายใจค่ะ

เรามา...ช่วยกัน....ดูแลน้อง...ในครรภ์ ...ร่วมกันนะคะ


ขอบคุณ ท่านอจ. หมอเปิ้น.... ขอเรียก ท่านว่า "อจ. แม่" นะคะ .... เดียว "เปิ้น" จะเปลี่ยนเลยนะคะ
ขอบพระคุณ อจ. แม่ มากๆๆนะคะ
เตรียมตัวขึ้นเวทีใหญ่ ตัวจริง เสียงจริง รักษาสุขภาพด้วย นะ พี่หมอ
ให้กำลังใจพี่เปิ้นนะครับ
ชอบตรงนี้มากเลยครับ
คุยปัญหาต่างๆๆ...ที่เธออยากเล่า ....เล่า...เพื่อเธอ จะได้ระบายและ...เธอสบายใจค่ะ
บางที การให้ที่ยิ่งใหญ่ อยู่ที่การฟังนี่เองนะครับ
ขอบคุณสาระดีๆ ที่นำมาฝากครับ
ขอบคุณ ทุกๆๆ ท่านมากๆๆนะคะ ... ดีใจมากที่สุด ... ที่ทุกๆๆท่านให้กำลังใจเช่นนี้ค่ะ ค่ะ
-สวัสดีครับพี่หมอ...
-มาร่วมเรียนรู้กับคุณแม่วัยใสครับ..
-เรียนรู้ไว้มาก ๆ เตรียมตัวเป็นคุณพ่อวัยใส 5555
-มีความสุขในการทำงานนะครับ..
-ชวนไปเรียนรู้เรื่่อง"ข้าว"ด้วยกันนะครับ..
ขอบคุณ น้องเพชร .... มากๆๆนะคะ ... "น้องทั้ง2 ท่าน สบายดี"
เป็นการทำงานที่มีรูปแบบดีๆ แสะมีอานิสงส์สูงมากค่ะ..
แวะมาส่งกำลังใจ คุณหมอคนเก่งค่ะ เพิ่งเคยเห็นคุณหมอใส่หมวกปีกกว้าง ตะลุยงานแบบนี้ค่ะ cheers!!!!
ขอบคุณพี่ใหญ่มากๆๆ ค่ะ เปิ้นดีใจมากๆๆ ค่่ะ พี่ใหญ่ มีเมตตาต่อเปิ้น ตลอดมานะคะ
ขอบคุณพี่ใหญ่มากๆๆ ค่ะ อากาศเปลี่ยนแปลเร็วมาก ดีแลสุขภาพ นะคะ
ขอบคุณมากค่ะ กับข้อ Comment ดีดีที่มีให้นะคะ ดีใจมากที่ท่าน ... คิดถึงและให้กำลังใจ หมอเปิ้น นะคะ...
เป็นตัวอย่างการทำวิจัยจากใจที่อยากช่วยเหลือ..ภาพแสดง structural equation model แสดงถึงที่มาทางวิชาการที่เข้มแข็ง ประทับใจวิญญาณครูของ อาจารย์วิ (ที่ท่านหันมาใช้คำกันเอง อย่างยายไอดิน..น่ารักอีกแบบคะ) ภาพนี้ดูง่ายสบายตาดี
เรียน ท่าน อจ. แม่ ... เปิ้น มีแบบให้ ท่านอจ. แม่ พิจารณา อีกแบบนะคะ